

Subcision: Cellulite Reduction
Subcision is a simple procedure to correct depressed cellulite lesions
- There is relationship between fibrous septa and depressed lesions, as shown in the literature
- Performed under local anesthesia, subcision is an outpatient procedure in which subcutaneous fibrous septa that pull the skin down are cut
- Good results are achieved with proper technique and when performed by experienced physicians
- The procedure is usually performed using a simple subcision needle and does not leave scars
- This procedure can be combined with other treatments for cellulite
- It can be repeated, if deemed necessary
Introduction
Originally described by Orentreich and Orentreich, subcision (‘subcutaneous incisionless surgery’) is a very simple surgical technique for the treatment of wrinkles and scars on the face. In 1995, Hexsel and Mazzuco developed this technique for the specific treatment of cellulite.
In clinical practice, approximately 80% of patients undergoing subcision for the treatment of cellulite are found to be very satisfied with the results. The first author, who has the largest experience in the world in this technique, having treated approximately 2000 patients and who described the technique for the treatment of cellulite, considers subcision to have the advantage of being a simple, minimally invasive, low cost technique with immediate, reproducible and persistent results in the treatment of depressed lesions of cellulite, without the risk of scar formation or significant side effects. Moreover, this technique addresses the fibrous septa, which are responsible for the depressions of cellulite.
Cellulite affects almost every woman. Although there are no precise data in different populations, prevalence higher than 90%. It most commonly affects thighs and buttocks, but it may also occur in the abdomen and arms. It is characterized by altered skin relief in the affected areas. Cellulite generally occurs after adolescence and tends to worsen with advancing age due to the superimposition of an aggravating factor: skin flaccidity. Another factor that aggravates this condition is the increased deposition of localized fat. Coincidentally, cellulite occurs in areas where a woman’s body naturally stores fat.
Anatomic bases of the depressed lesions and action mechanism(s)
Besides having a thicker layer of adipose tissue compared with men, women have larger and more rectangular fat lobes and perpendicular fibrous septa that attach the skin to the muscular fascia. These cause the projection of subcutaneous fat into the skin surface, thus causing the changes in relief typical of this condition: depressed lesions and raised areas.
It is noteworthy that cellulite mainly occurs in the areas of fat deposition in women, such as the buttocks, thighs, and outer thighs. In those areas where fat is stored, cellulite is more difficult to eliminate by dieting, except through extreme diets that promote an intense weight loss.
With the increased understanding of the pathogenesis and its relation to the most common feature seen in cell¬ulite, the depressed lesions caused by a subcutaneous septa that pulls the skin down, subcision has become the procedure of choice for the treatment of depressed lesions of cellulite, by cutting those subcutaneous fibrous septa. It is an outpatient procedure performed under local anesthesia, and acts by three mechanisms of action:
- Sectioning of the subcutaneous fibrous septa, thus releasing the tension on the skin in the area of the depressed lesions
- The formation of hematomas from sectioning of the accompanying vessel that is typically next to the subcutaneous septa, with subsequent fibroplasia, promoting a natural physiological filling of the lesions
- Redistribution of the traction forces produced by the subcutaneous septa and tension from the fat on the skin.
Patient selection
Patients eligible for subcision are those with evident depressed lesions in the affected areas (thighs and buttocks) that are visible without the use of any maneuver, such as pinching the skin or muscle contraction.
Expectations should be realistic as there is no improvement in skin flaccidity or localized fat after subcision – conditions frequently seen in patients with depressed lesions. The bruises often produced by treatment may take 30–60 days to disappear and patients should be made aware of this. Failure to adhere to pre-operative instructions may result in cosmetic complications that are difficult to treat, such as iron deposition and discoloration resultant from it.
Contraindications to the procedure include the presence of coagulation disorders or the use of medications that interfere with local anesthetics or with the process of coagulation, systemic diseases, systemic or local active infection, pregnancy, breastfeeding, and a history of keloids or hypertrophic scars.
As cellulite is a multifactorial condition, other measures are recommended to maintain the results including diet, exercise and weight control, among others.
Pre-operative instructions
Some instructions should be followed pre-operatively:
- Discontinue iron in medicines or food, for 1 month before the procedure.
- If possible, discontinue medications that interfere with blood coagulation, for 1–2 weeks before the procedure, such as nonsteroidal anti-inflammatory agents, ginkgo biloba, vitamin E and some hormones.
- Where present, treat possible local infections such as folliculitis.
- Do not undergo the procedure during the menstrual period.
Blood tests should be done 15 days before the procedure, including a coagulogram and other specific exams, according to the patient’s history and needs. Pay special attention to potential thrombophilia candidates (history of thrombosis, abortion, etc.).
Day of the procedure
As cellulite occurs in easily contaminated areas, the authors recommend the use of ciprofloxacin 500 mg twice a day for 3 days, starting 6 hours before the procedure. The authors also recommend acetaminophen 1 hour before and continued use, every 6 hours, for 2 days.
Photographs are taken.
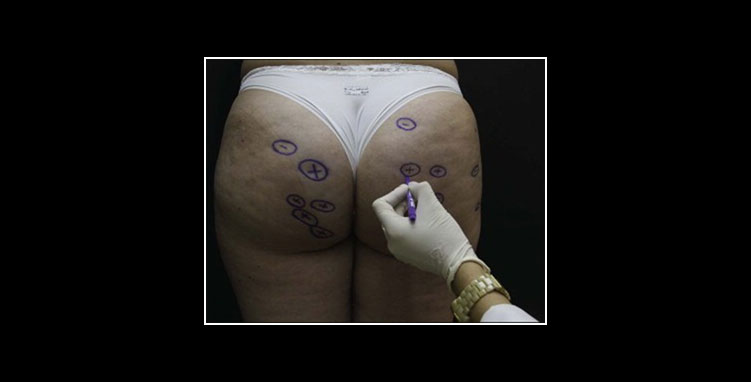
A physical examination should be performed in the standing position with relaxed muscles and with illumination from above in order to better view and mark the lesions to be treated with a surgical pen. It is recommended to select lesions 30 mm in diameter or smaller, or 30 mm portions of larger lesions, to avoid formation of hematomas and dissection planes that are too large and can potentially lead to complications.
Figure. Marking of the lesions suitable for subcision. The symbols ‘+’ highlight deeper lesions
REFERENCES
1. Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21:543–9.
2. Alam M, Omura N, Kaminer MS. Subcision for acne scarring: technique and outcomes in 40 patients. Dermatol Surg. 2005;31:310–7.
3. Savanth SS. Textbook of dermatologic surgery and cosmetology. 2nd ed. Mumbai: ASCAD; 2005. Is it only one author? Pitted facial scar revision; pp. 208–16.
4. Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45:109–17.
5. Khunger N. Standard guidelines of care for acne surgery. Indian J Dermatol Venereol Leprol. 2008;74:S28–36.
6. Al Ghamdi KM. A better way to hold a nokor needle during subcision. Dermatol Surg. 2008;34:378–9.
7. Al-Khenaizan S. Nokor needle marking: a simple method to maintain orientation during subcision. J Drugs Dermatol. 2007;6:343–4.
8. Balighi K, Robati RM, Moslehi H, Robati AM. Subcision in acne scar with and without subdermal implant: a clinical trial. J Eur Acad Dermatol Venereol. 2008;22:707–11.